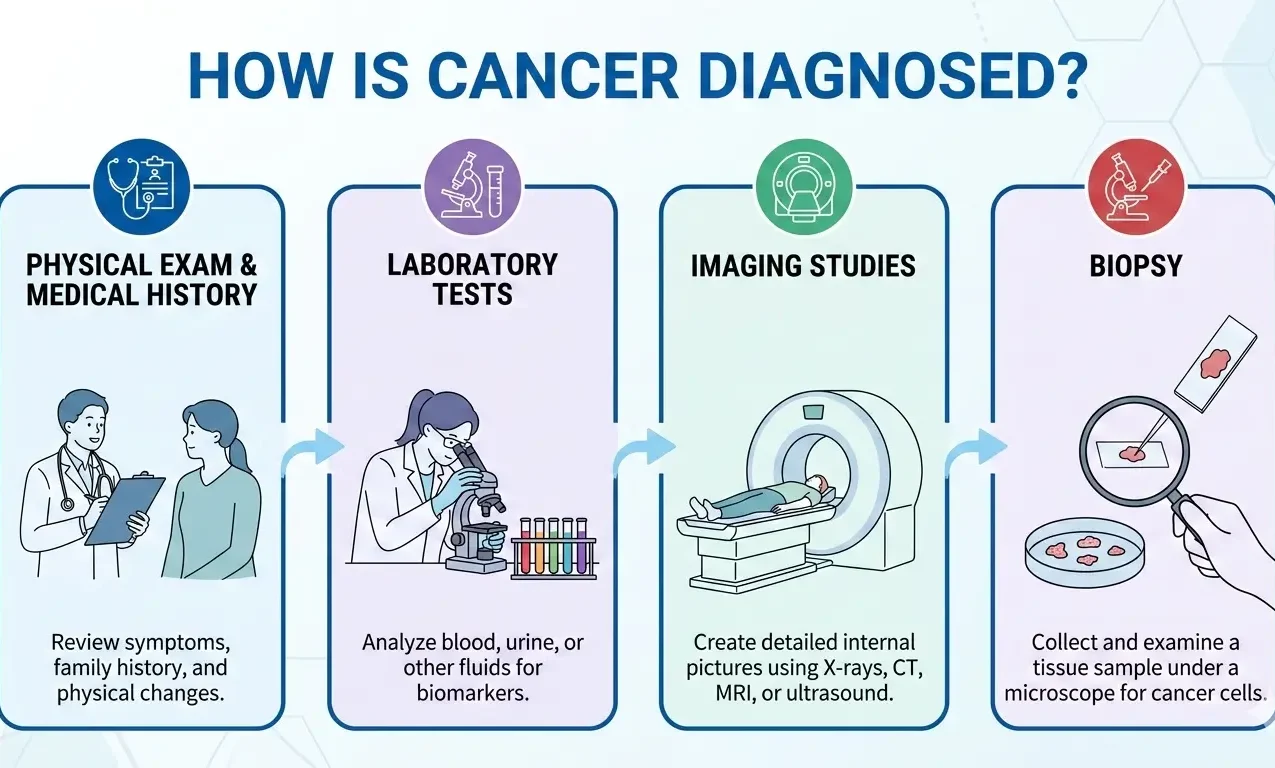
Finding out you might have cancer changes everything. It starts with a simple question: How do they check for cancer? Getting from a symptom to a real answer takes a few steps. Doctors use check-ups, machines, and lab tests to see if there are bad cells. Knowing how this works can make the process clearer and help you be more involved in your care.
Why Finding Cancer Early Matters
Table of Contents
ToggleBefore we talk about tests, it’s good to know that spotting cancer early can happen even without symptoms. Tests like mammograms and colonoscopies look for cancer when it’s easiest to treat. But if you have symptoms like losing weight for no reason, a cough that won’t go away, or strange lumps, the tests get more focused.
Clinical Evaluation: The First Step
Checking for cancer almost always starts with a check-up. This means two main things:
Your Health History- The doctor will ask about your health, what you do every day, and your family’s health. Because some cancers run in families, it helps to know if anyone else has had it. They’ll also ask about your symptoms, how long you’ve had them, and how bad they are.
Physical Examination- The doctor will check your body for anything odd, like lumps or bigger organs (like your liver or spleen). They’ll also look at your skin for changes in moles or spots. A physical exam can’t say for sure if it’s cancer, but it gives clues about what tests to do next.
Laboratory Tests
If the doctor finds something during the exam, lab tests are next. Blood and urine tests usually can’t find cancer by themselves (except for blood cancers like leukemia). But they give important details about how your body is working.
- Complete Blood Count (CBC): This measures the number of different types of blood cells. An abnormally high or low count of certain cells can indicate cancer.
- Tumor Markers: Certain cancers release substances into the blood called tumor markers. For example, the PSA test is used to monitor prostate health.
- Urinalysis: Checking urine for blood or specific proteins can help identify bladder or kidney issues.
Imaging Procedures
Imaging lets doctors see inside your body without cutting. These tests help find where a tumor might be and how big it is.
X-rays and Mammograms
X-rays are the most common form of imaging. Mammograms, which are specialized X-rays of the breast, are the gold standard for detecting breast cancer early.
CT Scans (Computed Tomography)
A CT scan takes a series of X-rays from different angles and uses a computer to create cross-sectional images of the bones, blood vessels, and soft tissues.
MRI (Magnetic Resonance Imaging)
Using powerful magnets and radio waves, an MRI produces detailed images of soft tissues, making it particularly useful for diagnosing brain tumors or spinal cord issues.
Ultrasound
Ultrasound uses high-frequency sound waves to create images of internal organs. It is frequently used to evaluate lumps that can be felt but not seen on an X-ray.
PET Scans (Positron Emission Tomography)
In a PET scan, a small amount of radioactive tracer is injected into the vein. Cancer cells, which use energy differently than healthy cells, “light up” on the scan, helping doctors see if a cancer has spread.
The Gold Standard: The Biopsy
While imaging and blood tests give strong hints, a biopsy is usually the only way to know for sure if it’s cancer. In a biopsy, they take a sample of cells and look at them under a microscope.
Types of Biopsies:
- Fine Needle Aspiration (FNA): A thin needle is used to withdraw fluid or small tissue fragments.
- Core Needle Biopsy: A slightly larger needle removes a “core” of tissue.
- Surgical Biopsy: A surgeon removes an entire lump (excisional) or a portion of a suspicious area (incisional).
- Endoscopic Biopsy: Using a thin, lighted tube (endoscope), doctors can see inside the body (like the colon or lungs) and take samples.
After taking the tissue, a pathologist checks the cells to see if they’re cancerous, what kind of cancer it is, and how fast it might grow.
Staging: Determining the Extent
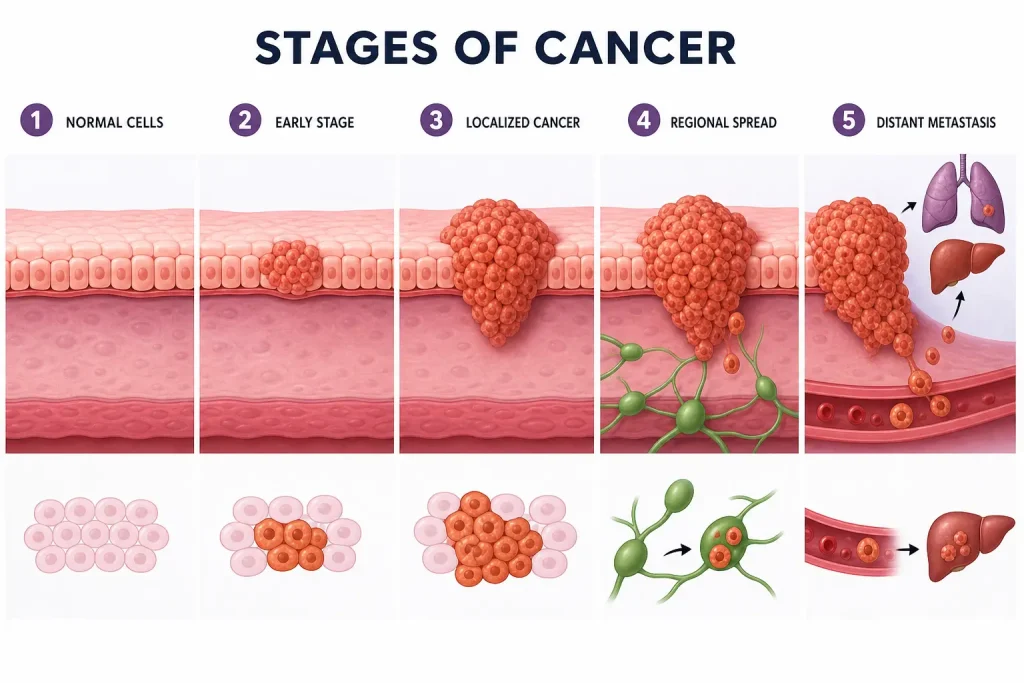
Once they know it’s cancer, the next step is staging. Staging tells how big the tumor is and if it has spread to lymph nodes or other places. This is super important for planning the right treatment. Doctors often use the TNM system:
- T (Tumor): Size and extent of the main tumor.
- N (Node): Whether the cancer has reached nearby lymph nodes.
- M (Metastasis): Whether the cancer has spread to distant organs.
Cancer Staging: The TNM System
The process of figuring out how big a tumor is and how far it has progressed throughout the body is formally known as cancer staging. Doctors use various advanced diagnostic tools—including detailed physical exams, sophisticated imaging tests (like CT scans, MRIs, and PET scans), and tissue biopsies—to precisely assign a stage.
The gold standard for most cancer types is the TNM system (Tumor, Node, Metastasis), which uses a combination of these three factors to categorize the disease:
- T (Tumor): Describes the size of the primary tumor and the extent to which it has invaded nearby tissue structures. This is often sub-categorized (e.g., T1, T2, T3, T4) with increasing severity. The specific T category (e.g., T1a vs. T1b) can provide microscopic details about the depth of invasion or specific tissue layers involved.
- N (Node): Indicates whether the cancer has spread to the nearby (regional) lymph nodes. The numerical code (e.g., N0, N1, N2, N3) reflects the number and location of involved nodes. Lymph nodes are a key battleground, as they are the first destination for cancer cells breaking away from the primary site.
- M (Metastasis): Confirms whether the cancer has spread (metastasized) to distant organs or parts of the body, a process called distant spread. This is a binary category (M0: no distant spread; M1: distant spread present). This factor is the most significant determinant of prognosis.
By combining the specific details of the T, N, and M factors, doctors categorize the cancer into stages 1 through 4, which offers a clear, international language for the disease’s status. It’s important to note that a separate category,
Stage 0 (Carcinoma in situ), is used to describe non-invasive cancer where abnormal cells are present but have not spread past the original layer of tissue.
Stage 1 Cancer – The Early, Localized Stage
Stage 1 represents early-stage cancer, where the disease is highly localized.
- Characteristics: The tumor is typically small and confined entirely to its organ of origin. Crucially, it has not spread to the lymph nodes (N0) or distant organs (M0). The specific designation will often be T1, N0, M0. The cancerous cells are typically well-differentiated, meaning they closely resemble healthy cells and are less aggressive.
- Prognosis and Treatment: Stage 1 is generally associated with the best prognosis and the highest cure rates. Treatment is often highly successful, typically involving Surgery to remove the tumor entirely with clean margins. In some cases, localized Radiation Therapy or Targeted Therapy may follow or supplement surgery, depending on the cancer type and specific risk factors for recurrence. Early detection through screening is paramount for catching cancer at this most manageable stage.
Stage 2 Cancer: Local Spread
In Stage 2, the disease has grown, signaling a more significant local presence than Stage 1, yet remains localized to the primary site or nearby tissues.
- Characteristics: The tumor is larger than in Stage 1 (T2), or it may have started to grow more deeply into adjacent tissues. It might also have spread to a few nearby lymph nodes (N1), or the lymph nodes might be microscopically involved. However, distant metastasis is still absent (M0). The cells might be moderately differentiated.
- Prognosis and Treatment: The tumor size and potential for occult local spread necessitate a more aggressive, multi-modality approach. Surgery is common, often followed by Chemotherapy and/or Radiation to eliminate any remaining microscopic cancer cells in the local area (adjuvant therapy). For some cancers, systemic therapy might be given before surgery to make the operation easier (neoadjuvant therapy). Stage 2 cancers still boast high survival rates when treated quickly and comprehensively.
Stage 3 Cancer: Regionally Advanced
Stage 3 signifies regionally advanced cancer, meaning the disease has a substantial local presence and significant lymph node involvement.
- Characteristics: The tumor is larger (T3 or T4), and the cancer has spread extensively to regional lymph nodes (N2 or N3), often several or in clusters, or has invaded nearby organs or structures. However, it has not yet traveled to distant organs (still M0). The cancer cells are often poorly differentiated, indicating more aggressive behavior.
- Prognosis and Treatment: The greater regional spread means a higher chance of recurrence. Treatment plans are complex and involve careful coordination among specialists (a multidisciplinary tumor board). Treatment choices frequently include a combination of Neoadjuvant Therapy (Chemotherapy, Radiation, or both given before surgery to shrink the tumor and treat micrometastasis), followed by Surgery (if feasible and margins can be cleared), and then Adjuvant Therapy (further Chemo, Radiation, Immunotherapy, or Targeted Therapy) to maximize eradication. The goal is to eliminate both the visible tumor and any residual disease in the surrounding area.
Stage 4 Cancer: Metastasis (Distant Spread)
Stage 4 is the most advanced stage, characterized by Metastasis, meaning the cancer has spread from its original site to other, distant parts of the body. This is defined by the M1 designation.
- Characteristics: The disease affects your whole body and is systemic. It often spreads to vital organs such as the liver, lungs, brain, and bones. The cancer cells are typically undifferentiated or highly aggressive. Symptoms may be more pronounced and severe due to the widespread disease burden.
- Prognosis and Treatment: Treatment at this stage is primarily palliative—aimed at controlling the disease, managing symptoms, prolonging life, and improving the patient’s quality of life, rather than achieving a definitive cure. Treatment Options are systemic and include Chemotherapy, Immunotherapy, Targeted Therapy, and Hormone Therapy. Localized treatments like surgery or radiation may be used to manage painful or problematic metastatic sites. Advances in modern oncology, particularly in immunotherapy and targeted therapy, have made it possible for many people with Stage 4 cancer to live longer, better lives, turning some cancers into chronic, manageable conditions.
- Re-Staging and Monitoring: After initial treatment, especially for more advanced cancers, doctors often perform re-staging to assess the treatment’s effectiveness. This post-treatment staging is crucial for monitoring remission or detecting recurrence. Regular surveillance scans and blood tests are essential for all cancer survivors.
Early Signs and Symptoms of Cancer: The Importance of Vigilance
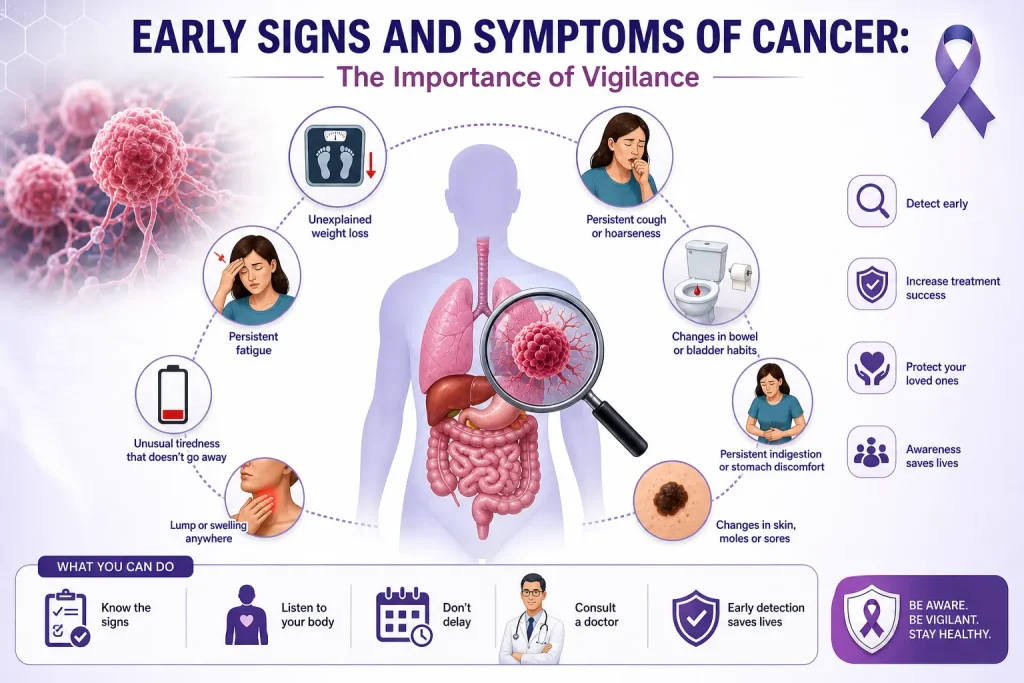
Early Signs and Symptoms of Cancer are often subtle and easy to ignore, but recognizing them at the right time can dramatically increase the chances of a favorable outcome. Catching cancer early can be life-saving because those first, vague signs are frequently missed. Cancer usually develops slowly, and your body often sends warning signals before the disease reaches advanced stages. Knowing what to look for allows for faster diagnosis, better care, and a significantly improved shot at remission or cure. Ignoring persistent changes can complicate treatment unnecessarily.
Common First Signs of Cancer (The “CAUTION” Signs)
The earliest signs of cancer depend heavily on its location and type, but certain persistent, unexplained changes are common across many malignancies. Both individuals and healthcare providers must maintain a high index of suspicion. Don’t ignore these vital health changes:
- Losing Weight Without Trying: An unexplained, significant loss of weight (more than 10 pounds, or 5% of body weight) over six months without a change in diet or exercise habits can be a sign of cancers of the stomach, lungs, esophagus, or pancreas, as the disease can disrupt metabolism and nutrient absorption. This is known as cancer cachexia.
- Feeling Tired All the Time (Persistent Fatigue): Extreme, pervasive tiredness that is not relieved by rest can be cancer-related. It is often linked to internal bleeding (e.g., colon cancer causing anemia due to iron loss) or blood cancers like leukemia, but can also be caused by the body’s ongoing immune response to the tumor. If you are always tired for no discernible reason, medical evaluation is necessary.
- Weird Bleeding or Discharge: Any bleeding that is abnormal for your body is a serious warning sign and requires immediate investigation to rule out malignancy:
- Gastrointestinal: Blood in your stool (melena or hematochezia) can signal colorectal cancer.
- Urinary: Hematuria (blood in the urine) can point to bladder or kidney cancer.
- Gynecological: Unusual vaginal bleeding (especially post-menopause, between periods, or after intercourse) is a red flag for uterine or cervical cancer.
- Pulmonary: Coughing up blood (hemoptysis) may indicate lung cancer.
- Integumentary: Nipple discharge (especially bloody or unilateral) or blood from another orifice.
- A Lump or Thickening: The discovery of a new lump in areas like the breast, neck (enlarged or firm lymph nodes), testicles, armpit, or groin requires immediate medical attention. A lump that is fixed, firm, and non-tender is generally more concerning than a soft, mobile one. While not all lumps are malignant, only a biopsy or definitive imaging can confirm.
- Skin Changes: Persistent changes to the skin should be investigated, as the skin is often a mirror for internal health:
- Melanoma: New moles or moles that change size, shape, color, or bleed (using the A-B-C-D-E rule for melanoma: Asymmetry, Border irregularity, Color variation, Diameter > 6mm, Evolution/change).
- Other Cancers: Skin turning darker (hyperpigmentation) or yellowish (jaundice—a sign of liver or pancreatic issues), persistent non-healing sores or ulcers, or chronic itchiness or redness in a localized area.
- Pain That Won’t Go Away: Unexplained, chronic pain lasting for weeks or months can be an early symptom, particularly if the tumor is pressing on nerves or bone. Persistent back pain, headache, or abdominal pain should never be dismissed without proper diagnostic workup, as it can be a sign of bone, brain, or ovarian cancer.
- Changes in Bowel or Bladder Habits: Long-term changes such as new-onset constipation, diarrhea, changes in stool caliber (narrowing—a classic sign of colorectal blockage), or persistent urinary frequency, urgency, or pain (dysuria) can signal colon, bladder, or prostate cancer.
- A Cough or Hoarse Voice That Won’t Go Away: A cough that persists for more than three weeks, especially a dry cough, or a lasting hoarseness or change in voice (dysphonia) can be a warning sign for lung or throat cancer, particularly in smokers or those with heavy occupational exposure.
- Trouble Swallowing (Dysphagia): Difficulty or pain (odynophagia) when swallowing that continues over time could point to throat or esophageal cancer and requires urgent evaluation. The feeling of food sticking is a significant symptom.
- Persistent Fevers or Night Sweats: Unexplained, persistent fevers or drenching night sweats, not related to an infection, can be a symptom of certain cancers, particularly lymphomas and leukemias.
When Should You See a Doctor?
A key component of early detection is maintaining awareness and seeking prompt medical advice. Do not hesitate to see a doctor if:
- Your symptoms last more than two weeks and are unexplained by a minor illness.
- Your symptoms progressively get worse over time.
- You experience unexplained bleeding or significant, unintentional weight loss.
- You have a known history of cancer in your family (genetic predisposition) or personal history of significant risk factors (e.g., long-term smoking).
Getting checked early can help catch things faster and significantly improve your chances of getting better. The medical approach will involve a comprehensive physical exam, blood work, and targeted diagnostic imaging to identify the cause of the persistent symptoms.
What Is Cancer? Causes & Treatment Overview
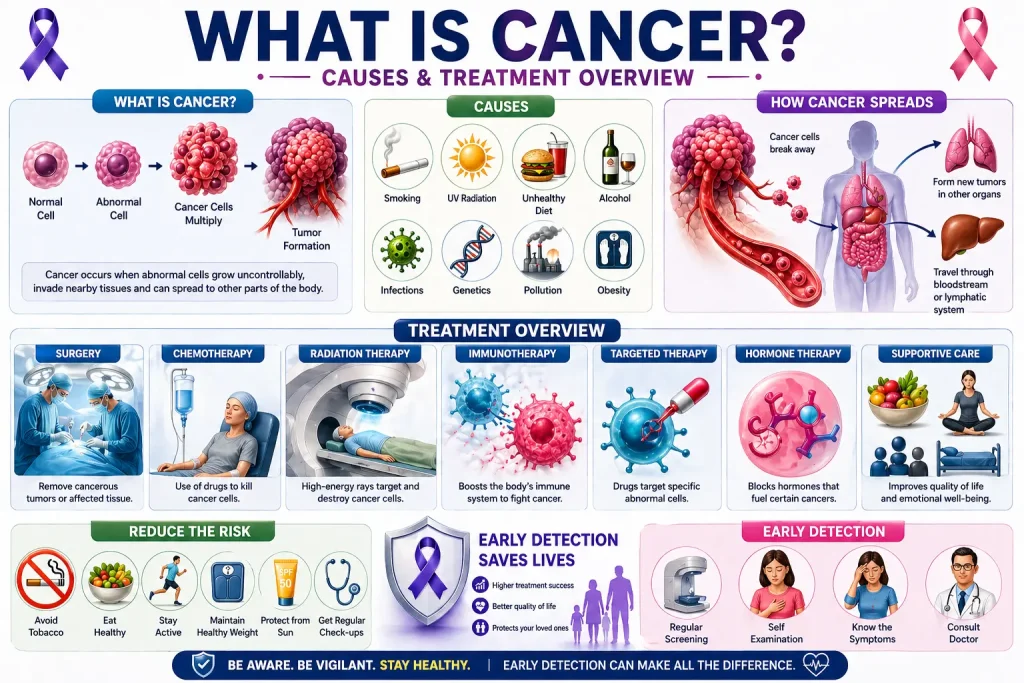
Cancer is not a single disease—it is a collective term for a group of conditions tied together by a fundamental glitch in the body’s natural processes: uncontrolled cell division. Normally, cells follow a strict life cycle, dividing to replace old or damaged cells and dying when worn out (apoptosis or programmed cell death). In cancer, cells ignore the usual signals to stop dividing or to die. They stick around, multiplying without order, leading to a dysfunctional proliferation of new cells where they shouldn’t be. This glitch in regulation leads to a cluster of growth, often forming a mass known as a tumor. Gaining clarity on cancer—its origins, signs, and treatment options—is the first step toward managing a diagnosis. The underlying problem is damage or mutations to the cell’s DNA, which controls growth and division.Benign vs. Malignant Tumors
Tumors are categorized into two primary forms, which dictates the necessary medical response:
- Benign Tumors: These non-cancerous growths are generally slow-growing and remain localized to their point of origin, encapsulated by surrounding tissue. They rarely pose a life threat and often do not recur after removal. Example: Uterine fibroids or common moles. However, a benign tumor in a critical area (like a pituitary adenoma in the brain) can still cause serious health issues due to mass effect.
- Malignant Tumors (Cancer): These are cancerous. They grow rapidly and aggressively, invading surrounding healthy tissues and organs. A critical feature of malignancy is metastasis—the process where cells break away from the primary tumor, enter the bloodstream or lymphatic system, and travel to form secondary tumors in distant locations. Malignant cells are also characterized by angiogenesis (the ability to form their own blood supply) and immortality.
Common Causes and Risk Factors: The Genesis of Cancer
While the precise reason for the onset of any single cancer often remains uncertain, most cases arise from accumulated gene changes (mutations) acquired during a person’s lifetime. These mutations affect key genes known as proto-oncogenes (which, when mutated, become hyperactive oncogenes that promote growth) and tumor suppressor genes (which, when inactivated, lose their ability to halt abnormal growth). Only a small percentage (about 5-10%) are caused by inherited germline gene mutations. These acquired or inherited changes can be triggered by a variety of interacting factors:
- Lifestyle Factors (Modifiable Risk Factors): These are the most controllable factors:
- Tobacco Use: The single most preventable cause of cancer, linked to at least 15 different cancer types, including lung, mouth, throat, bladder, and pancreatic cancers.
- Diet and Obesity: High-fat, low-fiber diets, and a sedentary lifestyle increase chronic inflammation and alter hormone levels, thereby increasing the risk for colon, breast, endometrial, and pancreatic cancers. Maintaining a healthy weight is vital.
- Alcohol Consumption: Excessive drinking is a risk factor for liver, breast, esophageal, and head and neck cancers, with risk increasing with the amount consumed.
Environmental Exposures (External Agents):
- UV Radiation: Excessive sun exposure or tanning beds is the main cause of skin cancer (melanoma, basal cell, and squamous cell carcinoma).
- Chemicals and Toxins: Occupational exposure to substances like asbestos (mesothelioma), benzene (leukemia), arsenic, or radon can cause mutations. Air pollution is also an increasing risk factor.
- Infections: Certain viruses and bacteria are responsible for up to 20% of global cancer cases. Examples include the Human Papillomavirus (HPV) (cervical, anal, throat cancers), Hepatitis B and C (liver cancer), and Helicobacter pylori (stomach cancer).
Genetics and Family History:
Inherited mutations in specific genes (like BRCA1/2 for breast and ovarian cancer, or genes linked to Lynch Syndrome for colorectal cancer) can significantly increase lifetime risk. Genetic counseling and testing may be necessary for those with a strong family history. However, having an inherited mutation does not guarantee cancer, only an increased predisposition.
Age: Age is the single biggest risk factor, as the accumulation of cell damage and mutations increases over a lifetime.
Modern Treatment Options: A Multidisciplinary Approach
Modern cancer care involves a multidisciplinary team (oncologists, surgeons, radiologists, pathologists) and often employs a combination of therapies tailored to the specific molecular profile and stage of the cancer.
- Surgery: The primary and often oldest method for treating localized cancer. If the tumor is contained, surgical removal can be curative. It is commonly used for solid tumors like breast, colorectal, and skin cancers.
- Chemotherapy (Chemo): Uses powerful cytotoxic drugs administered systemically (via blood) to kill fast-growing cancer cells throughout the body by interfering with cell division. While effective, it also affects some healthy, fast-dividing cells (e.g., hair follicles, bone marrow), leading to side effects.
- Radiation Therapy: A targeted approach that uses high-energy beams (e.g., X-rays, protons) to damage the DNA of cancer cells, preventing them from dividing. It is often used to shrink tumors before surgery (neoadjuvant), to eliminate residual cancer cells afterward (adjuvant), or to relieve pain (palliative). Techniques like IMRT and proton therapy allow for highly precise delivery.
- Targeted Therapy: A newer class of drugs that focuses on specific molecular abnormalities (targets), such as specific proteins, receptors, or signaling pathways, unique to cancer cells, leaving most healthy cells unharmed. Examples include drugs that block growth signals or inhibit blood vessel formation within the tumor (angiogenesis inhibitors). These are often guided by molecular testing of the tumor.
- Immunotherapy: This revolutionary approach sharpens the body’s own immune system to recognize and attack cancer cells. Instead of directly attacking the tumor, it removes the “brakes” the cancer puts on the immune response (Checkpoint Inhibitors), turning the patient’s defenses into smarter, more effective hunters. This treatment has revolutionized the care of melanoma, lung, and several other cancers.
- Hormone Therapy: Used for hormone-sensitive cancers (like estrogen-receptor-positive breast cancer and prostate cancer), this treatment blocks the body’s natural hormones from reaching and feeding the cancer cells or lowers the overall hormone levels in the body.
- Stem Cell Transplant: Primarily used for blood cancers (leukemia, lymphoma), this treatment replaces diseased bone marrow with healthy stem cells.
Prevention and Early Detection
Effective cancer management focuses on both primary prevention (reducing risk factors) and secondary prevention (early detection).
- Primary Prevention: Adopting a healthy lifestyle (avoiding tobacco, maintaining a healthy weight, limiting alcohol, and eating a nutritious diet) and utilizing prophylactic vaccines (e.g., HPV vaccine to prevent cervical and other cancers, and Hepatitis B vaccine to prevent liver cancer) can drastically reduce the risk of developing many types of cancer.
- Early Detection Screenings: Routine check-ups like mammograms (breast cancer), colonoscopies (colorectal cancer), Pap smears (cervical cancer), and PSA tests (prostate cancer, though debated) can find cancer before symptoms even appear, often catching it at Stage 1 or 2, which greatly improves the chances of cure and necessitates less-intense treatment.
Genetic Testing and Molecular Analysis
Now, checking for cancer means more than just finding the type. Molecular tests look at the DNA and proteins inside the cancer cells. This helps doctors figure out the specific things that are making the cancer grow. Then, they can use Targeted Therapy—a treatment made just for your cancer’s genes.
Conclusion
Understanding how cancer is diagnosed is the first step in navigating a complex medical landscape. From the initial physical exam and blood work to advanced imaging and the definitive biopsy, each step is designed to provide a clear picture of what is happening inside the body. While the process can be overwhelming, these diagnostic tools are more precise than ever, allowing for earlier detection and highly personalized treatment strategies. If you have concerns about your health or need to schedule a screening, please visit our Home page or visit our Contact Us page to speak with a specialist
How Consult Grab Helps You Choose the Best Cancer Treatment In Delhi?
Finding the right cancer treatment center and doctor can be hard, especially when your health and time are on the line. Consult Grab makes this process easier by giving patients in Delhi and the surrounding areas personalised advice and expert help. People can do the following with Consult Grab:
- Connect with Top Oncologists in Delhi: You can find highly qualified cancer specialists who can help you with your specific type of cancer and treatment needs.
- Compare Treatment Options: Learn about the differences between hospitals, therapies (like surgery, chemotherapy, radiation, and immunotherapy), and what you can expect from each one.
- Get Personalised Help: Get help with making appointments, getting ready for consultations, and understanding treatment plans so you can make smart choices.
- Consult Grab makes the whole process easier, from getting expert advice to setting up appointments. This lets you focus on your health and recovery.
Disclaimer
The information provided in this article is generated for informational purposes only. The content is created with the help of general medical knowledge and data available on the internet. It should not be considered as professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional or specialist for proper medical guidance and personalized treatment recommendations